
David McCarthy teaches in the Risk Management and Insurance program at the University of Georgia. Previously he worked with a large life insurance company in his native South Africa; taught at Oxford University and Imperial College, London; and advised the National Treasury of South Africa on financial sector regulation and pensions. He earned his PhD at the Wharton School of the University of Pennsylvania.
For millennia, people have wondered whether there is a maximum limit for the human lifetime, and if so, what it is. Historical estimates of the maximum strongly suggest that it has risen over recorded history, but the current record (though disputed) has not changed for 25 years. Some researchers have asserted that this is because the maximum human lifespan is limited by immutable biological factors.
My coauthor, Po-Lin Wang, and I have been working on human mortality for many years with a focus on the financial implications of mortality changes for governments and financial intermediaries such as pension funds and insurance companies. More recently, we realized that our work, when applied to national mortality data for 19 currently-industrialized countries from the Human Mortality Database (HMD), could provide new insights on this age-old and important question.
Mortality compression vs mortality postponement
Our newest study, unlike most prior mortality research, grouped the data by year of birth, rather than the more usual year of death, so we could examine how mortality between the age of 50 and 100 changed across birth cohorts. Nearly 200 years ago, Benjamin Gompertz first noticed that at older ages, mortality increases by a roughly constant percentage with each year of age, now called the Gompertz Law. This regularity allowed us to summarize the entire mortality experience of each birth cohort with just two numbers: their initial level of mortality at age 50, and the average rate of increase in mortality experienced as they aged. If the oldest humans are pushing at a biological limit to lifespan, we would expect that, as mortality at age 50 falls, the rate of increase of mortality with age should rise, so that the biological maximum is preserved at the same age.
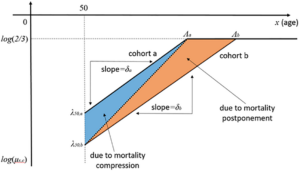
Demographers call this pattern mortality compression, because it will result in the distribution of age at death being increasingly compressed below the biological maximum. But if the rate of increase of mortality with age doesn’t change, or even falls, as age-50 mortality falls, the distribution of age at death will simply shift to the right, or even spread out, a pattern called mortality postponement. Figure 1 illustrates how we used this method to divide changes in mortality patterns across different cohorts between compression and postponement (the figure uses a logarithmic scale for the vertical axis, so a constant percentage increase in mortality with age shows up as a straight line).
Figure 1: The division of changes in cohort mortality between compression and postponement
Case study: Swedish females
Sweden has the longest data series in the HMD, having collected vital statistics since 1750. Accordingly, we focus on results for Swedish females. Figure 2 shows the change in remaining life expectancy at age 50 for Swedish females born 10 years apart, in years, divided into the portion due to compression (blue) and the portion due to postponement (red). We also show 95% confidence intervals for each part, and dots represent the actual change in observed life expectancy (slightly different from the sum of the two components because the Gompertz law is not an exact fit). Clearly, for most of the recorded data, the blue bars, but not the red ones, are usually statistically different from zero, indicating that mortality compression was, in fact, the dominant pattern of mortality improvement.
Figure 2: Changes in remaining life expectancy (years, vertical axis) between cohorts born 10 years apart (birth year of second cohort on the horizontal axis). Red bars indicate portion due to postponement, blue bar portion due to compression. Dots represent the true change in life expectancy; 95% confidence intervals shown.
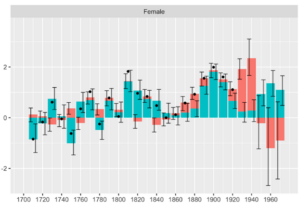
Nevertheless, there were occasional episodes of mortality postponement, when the red bars are significantly different from 0. One such episode affected Swedish females born between 1860 and 1890, but by far the most dominant one in our data is being enjoyed by females born between 1910 and 1940 (ie. those currently between 80 and 110 years old).
We then estimated the statistical distribution of the age at death of the longest-lived person in each birth cohort (shown in grey in Figure 3), and the age at which the mortality rate of people in each cohort first reached one half (shown in red). (Prior work suggests that around that mortality rate, the Gompertz law ceases to apply and mortality rates plateau and there is some theoretical justification for this). Black dots in the figure show the oldest-lived people in each cohort where data were available from two publicly-available international databases of centenarians.
Figure 3: 95% confidence intervals for the length of life of the oldest person in each birth cohort (grey) and the age at which annual mortality probabilities first reach one half (red). Dots show the actual oldest person in each birth cohort, where data is available.
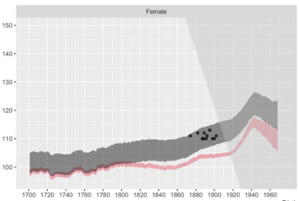
As can be seen from the red bar in the figure, the age at which Swedish females first reached a mortality probability of one half was almost constant, around 100, for those born between 1700 and 1860: the dominant pattern for these birth cohorts was mortality compression. But by the cohort of 1890, it had risen to 105 and remained at that level until the birth cohort of around 1918 (who are currently age 105). The diagonal line in the figure separates the past from the future. We project that this age will rise further – and dramatically – for those born after 1918. Of course, these cohorts are still too young to break longevity records.
The figure also shows that the observed maximum age at death of individuals in each cohort (the black dots) lie within our estimated distribution for that quantity (the grey bar). The distribution of the maximum age at death rises above the red bar because the maximum age at death is affected both by population size and by underlying mortality. The population of Sweden has risen over the period, and the more people there are, the more likely it is that one of them will reach an advanced age, even if the underlying mortality rates are the same.
The rest of the world
The patterns illustrated using Swedish females are broadly shared by males and females across all the countries we examined. The dominant pattern of mortality improvement appears to be mortality compression, interspersed with bursts of mortality postponement. The first postponement episode occurred for those born at the end of the 19th century (timings differed by country and birth sex; it typically was stronger and occurred sooner for females). By far the most prominent of these is currently being experienced by cohorts born roughly between 1910 and 1940 (with some country differences) who reached age 50 between 1960 and 1990.
Implications
Our work shows that mortality records have been slow to increase, not because the human lifespan has reached a biological limit, but rather because the cohorts currently experiencing significant mortality postponement are still too young to break longevity records. If our projections are correct, this suggests that mortality records will rise dramatically in the coming decades. Thus, Japanese females (the oldest of whom recently died at age 119), are at the forefront of this transition.
This pattern will clearly have implications for public finance, including the US Social Security system. What about the consequences of our findings for individuals’ lives? First, while much has been written about the falling US life expectancy, readers should be aware that this is caused primarily by issues affecting young people (suicide, opioid addiction, gun violence). In recent decades, the mortality of older people in the US has been improving at rates not seen since the period following the introduction of Medicare in 1965, and older people in the US now have remaining life expectancies very similar to their peers of the same age in Europe.
Second, while our work suggests that there may be someone who reaches these advanced ages, it is unlikely to be any given individual. (In the US, the chance of you reaching these ages is roughly the same order of magnitude as the probability of you being struck dead by lightning this year). Therefore, the significance of our work for most readers is that, rather than dying at age 85 or 90 as you perhaps expected, you may live until 90 or 95. Prudent people should lengthen their planning horizons accordingly. If you are coming up to retirement and are able to do so, consider delaying taking social security, working longer (or part-time after you retire, if you can), and saving more.
Third, readers should be aware that people may live for 40+ years after they retire. Besides making adequate financial plans, they should also give some thought to how they can remain active, engaged, and connected to their families and communities. This will help ensure that what could be a very long stage of our lives will be as enjoyable and fulfilling as possible.
Above all, these longer lifespans bring tremendous opportunities, and people should do what they can to put themselves in a position where they can make the most of the opportunities that longer lives provide. Who knows: with luck, you may even be one of the vanishingly few people in human history who are given the opportunity to meet their great-great grandchildren!
Views of our Guest Bloggers are theirs alone, and not of the Pension Research Council, the Wharton School, or the University of Pennsylvania.